Gastro Esophageal reflux disease and current Understanding of Management Strategies
 Dr. Harsh Kapoor
Dr. Harsh KapoorMD, FRCP (Canada), FACP, FACG (USA),
Canadian Board Certified in Internal medicine and Gastroentrology
Fellowships in Gastroentrology, interventional ERCP (Canada)
and Liver Transplant Hepatology,
Prior-Associate Prof,Emory School of Medicine,Atlanta-Georgia (USA).
Chairman and Sr. Consultant
Institute of Digestive and Hepatobiliary Sciences
Primus Super Speciality Hospital-New Delhi
Most common problem in all parts of the word normal people gets symptoms 5 times/ months.It costs 1 billion dollars in North America to deal with treatment cost of drugs. Surgical treatment and manpower work loss due to this disease.Most common symptoms include sour taste in mouth, retrosternal burning, epigastric
discomfort post prandially. Some symptoms include ear infections, bad breath, recurrent sore throat, atypical chest pains which some times require a lot of investigations to prove as non cardiac. There are also sore throat, atypical chest pains which some times require a lot of investigations to prove as non cardiac. There are also ease of non productive cough, exacerbation of Bronchial asthma and sudden wakening up at night due to micro aspiration of gastric contents due to reflux. (short of breath)- Gastroesophageal reflux is a normal physiological phenomina and normally a healthy person gets 14 times a day gastric contents come to esophagus and pushed back with no side effects. Only patients who get symptomatic are those in whom gastric contents stays in the esophagus for > 5 min. and pH of the contents is < 4.
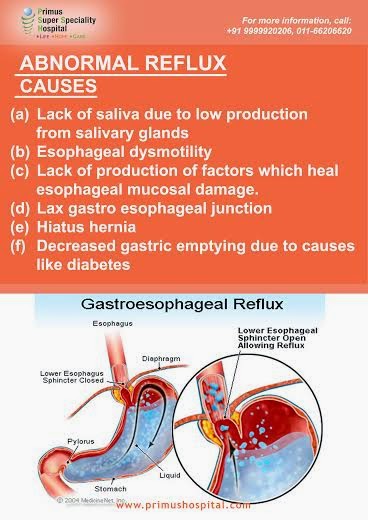
(a) Lack of saliva due to low production from salivary glands
(b)Esophageal dysmotility
(c) Lack of production of factors which heal esophageal mucosal damage.
(d) Lax gastro esophageal junction
(e) Hiatus hernia
(f) Decreased gastric emptying due to causes like ? diabetes
COMPLICATIONS OF REFLUX
Disturbed life style
Esophagitis
Esophageal strictures
Barretts esophagus
Esophageal cancer
INVESTIGATIONS –
Tests that can help us to confirm that the symptoms in question are due to Gastro esophageal reflux are:
(a) Upper endoscopy – to see any esophagites. Hiatus hernia which may be contributing to the symptoms.
(b)Esophageal motility studies – to see any esophageal movement disorder.
(c)24 hr pH monitoring test to see symptoms co-relating to reflux and their pH at that point. Newer techniques for doing 24 hour pH monitoring where we do not have to insert catheter from nose which is very irritating are available – BRAVO.
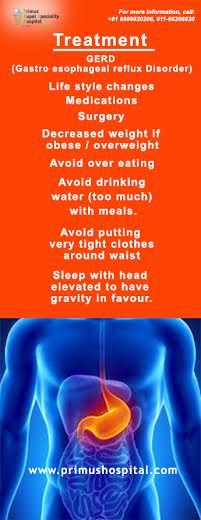
Treatment
(a) Life style changes
(b)Medications
(c) Surgery
Change in life style
- Decreased weight if obese / overweight
- Take meals in sitting position and not to lie down in the bed for 2 hr after eating.
- Avoid over eating
- Avoid drinking water (too much) with meals.
- Avoid putting very tight clothes around waist.
- Avoid carbonated drinks, chewgums (cause aerophasia), oily and spicy foods
- Sleep with head elevated to have gravity in favour.Medications H2 blockers – Old Rx, less effective and are out of favour now.Proton pump inhabitor– Omeprazole, Pantocid, Neksium like drugs, blocks production of acid to the 75-88% and very effective. Step down approach i.e. starting 1 tablet twice a day and after 8 weeks decrease to once a day for 4 weeks and then try to stop. If it is effective and after stopping rebound phenomena is seen then maintenance therapy on long term or on demand therapy is indicated.
Prokinetics – Due to cardiac side effects drugs like cysapride were taken off the shelf, but
 new generation drugs of this class, Kinapride, Lesuride etc. and some of the old drugs
new generation drugs of this class, Kinapride, Lesuride etc. and some of the old drugsDomperidone Mexran, Metocholor- Propamide are helpful if used judiciously.
Antacids – Drugs like Digene are helpful and are taken for symptomatic relief, i.e. post prandially. These are safe but no effect on the disease process.
Surgical treatment
Nissen fundoplication – I personally recommend in patients who either have no response to maximum dose of drugs or their symptoms are making life disrupted to great extent. This can also be considered if patient can’t afford drugs on long terms or have large hiatus hernia with esophagitis, non responsive to medical treatment;
Limitations - Fundoplication some times can cause dysphagia which might need balloon dilatation endoscopically after surgery.
- Dysphagia due to esophageal dysmotility if esophageal motility studies not done prior to surgery. Some times surgery may have to be undone.
- Nissen fundoplication may give away in 6-7 years in some patients.
Prerequisites prior to nissen fundoplication
- 24 hr pH monitoring – to prove symptoms due to reflux
- Esophageal motility studies to make sure so no motility disorders present. In the event esophageal dysmotility is noted then Nissen fundoplication is contra indicated.
In conclusion – Gastro esophageal reflux is a simple controllable disease. If neglected it can make life hell and also can lead to esophageal cancer which can be fatal.


Comments
Post a Comment